Wolff–Parkinson–White syndrome
Background
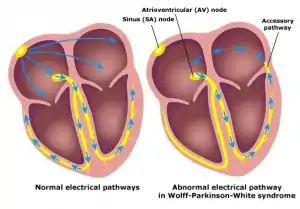
Graphic representation of the bundle of Kent in Wolff–Parkinson–White syndrome
- Abbreviation: WPW
- Congenital pre-excitation syndrome
- Presence of an accessory electrical pathway between atria and ventricles predisposing to supraventricular tachycardia
- Associated with certain genetic predispositions, Ebstein anomaly, and hypokalemic periodic paralysis[1] [2]
Types by Aberrant Pathway Site
- Type A
- Type B
Types by Cycle Direction
- Orthodromic
- Accessory pathway with retrograde reentry conduction
- Most common variant (~95% of cases)
- QRS narrow (delta wave absent)
- Referred to as 'concealed' accessory pathway [7]
- May see ST depression, TWI
- Rate 150-250 bpm
- Antidromic
- Accessory pathway with anterograde reentry conduction
- Least common variant (~5% of cases)
- QRS wide, delta wave present
- Rate 160-220 bpm, regular
Atrial Fibrillation and Flutter[8]
- Atrial fibrillation in up to 20% of patients with WPW
- Irregular rhythm, wide QRS complexes
- Changing QRS complexes in shape and morphology
- Axis remains stable as opposed to polymorphic VT
- Atrial flutter in ~7% of patients with WPW
- Similar features to atrial fibrillation with WPW
- Except regular rhythm
- Easily mistaken for monomorphic ventricular tachycardia
- Note that if unclear, always safest to assume VT and treat with shock
- Treatment with AV nodal blocking agents (adenosine, beta-blockers, calcium-channel blockers, amiodarone, digoxin) may incite ventricular fibrillation or ventricular tachycardia
- "Manifest WPW" = degeneration into VT or VF
Clinical Features
- Suspect in any patient with ventricular rate >300
- Many are asymptomatic
Infants
- Irritability, feeding intolerance
- CHF
- Intercurrent febrile illness
Children
- Chest pain, palpitations
- Shortness of breath
- Syncope/near-syncope
Adults
- Sudden onset "racing heart"
Differential Diagnosis
Narrow-complex tachycardia
- Regular
- AV Node Independent
- Sinus tachycardia
- Atrial tachycardia (uni-focal or multi-focal)
- Atrial fibrillation
- Atrial flutter
- Idiopathic fascicular left ventricular tachycardia
- AV Node Dependent
- AV Node Independent
- Irregular
- Multifocal atrial tachycardia (MAT)
- Sinus tachycardia with frequent PACs, PJCs, PVCs
- Atrial fibrillation
- Atrial flutter with variable conduction
- Digoxin Toxicity
Wide-complex tachycardia
Assume any wide-complex tachycardia is ventricular tachycardia until proven otherwise (it is safer to incorrectly assume a ventricular dysrhythmia than supraventricular tachycardia with abberancy)
- Regular
- Monomorphic ventricular tachycardia
- PSVT with aberrant conduction:
- PSVT with bundle branch block^
- PSVT with accessory pathway
- Atrial flutter with bundle branch block^
- Sinus tachycardia with bundle branch block^
- Accelerated idioventricular rhythm (consider if less than or ~120 bpm)
- Metabolic
- Irregular
- Atrial fibrillation/atrial flutter with variable AV conduction AND bundle branch block^
- Atrial fibrillation/atrial flutter with variable AV conduction AND accessory pathway (e.g. WPW)
- Atrial fibrillation + hyperkalemia
- Polymorphic ventricular tachycardia
^Fixed or rate-related
Palpitations
- Arrhythmias:
- Non-arrhythmic cardiac causes:
- Psychiatric causes:
- Panic attack
- Anxiety
- Somatic Symptom Disorder
- Drugs and Medications:
- Alcohol
- Caffeine
- Drugs of abuse (e.g. cocaine)
- Medications (e.g. digoxin, theophylline)
- Tobacco
- Misc
Evaluation
Workup

Delta wave
- ECG
Diagnosis

12 lead electrocardiogram showing classic findings
Although the ECG and an electrophysiology study are diagnostic, the characteristic features are not always seen on ECG
- Short PR interval - <0.12sec
- Due to loss of normal AV node conduction delay
- Differentiate from premature junctional complex
- Delta wave / slurred upstroke
- Due to early activation of ventricular myocardium
- QRS duration > 0.10 sec
- Represents a fusion beat
- Dominant R wave in V1, Type A WPW
- Left sided accessory pathway
- Dominant S wave in V1, Type B WPW
- Right sided accessory pathway
- Tall R waves in V1-V3 with T wave inversion
- Mimic RVH
- "Negative" delta waves in III and aVF
- Appear as pseudo-infarct Q waves
- Mimics prior inferior infarct
Management
Orthodromic
Treat like paroxysmal SVT
- Unstable
- Cardioversion (synchronized)
- Adult: 50-100 J
- Peds: 0.5-2 J/kg
- Stable
- Calcium channel blockers, beta-blockers, procainamide, or adenosine
- Procainamide is safest, as safe irrespective of type of pathway conduction
Antidromic
Treat like ventricular tachycardia
- Synchronized cardioversion
- Adult: 50-100 J
- Peds: 0.5-2 J/kg
- Procainamide (see page for dosing guidelines)
- Avoid if prolong QT or CHF
- Amiodarone with 'ABCD' drugs ie adenosine, beta-blockers, calcium-channel blockers, digoxin
- Wide-complex, irregular (presumed preexcited A-fib)
- Unsynchronized cardioversion (200J)
Atrial Fibrillation and Atrial Flutter
- Stable
- Procainamide 20-50 mg/min until arrhythmia suppressed
- Synchronized cardioversion, 100 - 200 J
- Unstable - synchronized cardioversion
- Consider higher joule dosage and frequency of repeats than for stable
- Avoid AV nodal blocking agents
Disposition
Discharge
- Consider if dysrhythmia was easily terminated and can arrange outpatient EP study with possible RF catheter ablation
- Consider consulting cardiologist regarding outpatient beta-blockers vs. more potent medications (amiodarone, sotalol, flecainide, etc.)
Admit[9]
- Patients with chest pain, CHF, electrolyte imbalance, or required cardioversion
- Syncope
- Uncertain diagnosis (wide-complex tachycardia)
- Significant associated structural heart disease (MVP, cardiomyopathy)
- Family history of Sudden cardiac death
- Atrial flutter or atrial fibrillation
See Also
External Links
References
- https://rarediseases.org/rare-diseases/wolff-parkinson-white-syndrome/
- https://patient.info/doctor/wolff-parkinson-white-syndrome-pro
- https://patient.info/doctor/wolff-parkinson-white-syndrome-pro
- https://emedicine.medscape.com/article/159222-workup#c8
- https://patient.info/doctor/wolff-parkinson-white-syndrome-pro
- https://emedicine.medscape.com/article/159222-workup#c8
- https://emedicine.medscape.com/article/159222-workup#c8
- Burns E. Wolff-Parkinson-White Syndromes. Life in the Fast Lane. http://lifeinthefastlane.com/ecg-library/pre-excitation-syndromes/.
- Ellis CR et al. Wolff-Parkinson-White Syndrome Treatment & Management. eMedicine. Dec 4, 2015. http://emedicine.medscape.com/article/159222-treatment#showall.
This article is issued from Wikem. The text is licensed under Creative Commons - Attribution - Sharealike. Additional terms may apply for the media files.