
CPR on Television
I don't know how many times I've seen CPR done on television where the patient immediately wakes without exhibiting any major outward signs of the effects caused by either the cause of the cardiac arrest or the CPR itself.
In the real world, this is very, very often not the case.
While there are some aspects of CPR as shown on television which are correctly portrayed, there are also some which are incorrect or at least inaccurate. Whether this is done for dramatic purposes or due to lack of knowledge on the subject is up for debate.
For the purposes of this answer, it will be much easier if we assume that all CPR done on television is done correctly.
The science...
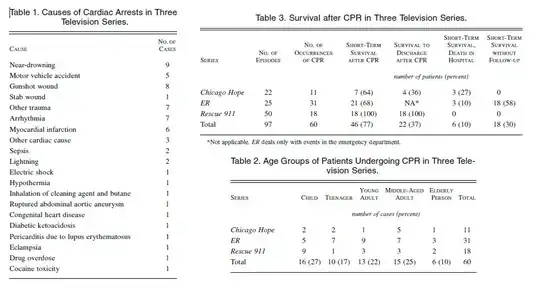
A paper studying depictions of CPR in 3 different (Rescue 911, ER, Chicago Hope) American television programs states quite clearly:
The survival rates in our study are
significantly higher than the most
optimistic survival rates in the
medical literature, and the portrayal
of CPR on television may lead the
viewing public to have an unrealistic
impression of CPR and its chances for
success. Physicians discussing the use
of CPR with patients and families
should be aware of the images of CPR
depicted on television and the
misperceptions these images may
foster.source
The breakdown of this study by victim is as follows:
A more recent study examined 26 episodes of Casualty, Casualty, 25 episodes of Holby City, 23 episodes of Grey's Anatomy and 14 episodes of ER screened between July 2008 and April 2009 and came to a similar conclusion.
Whilst the immediate success rate of
CPR in medical television drama does
not significantly differ from reality
the lack of depiction of poorer medium
to long term outcomes may give a
falsely high expectation to the lay
public. Equally the lay public may
perceive that the incidence and likely
success of CPR is equal across all age
groups. source
Already we can see that research indicates a sharp disparity between the effectiveness of CPR in reality and on film. Survey data cited by the Robert Wood Johnson Foundation further indicates that:
The public seriously overestimates
CPR's effectiveness. A survey that
included health care workers found
that those who were over 65 years old
predicted a 59 percent survival rate
for a person treated with CPR. People
under 30 were even more optimistic,
predicting a 75 percent survival rate.
source
This data sheds light on the fact that the success rate of CPR may not only be misrepresented by the media but by the textbooks as well...
Even more troubling, the surveyors
found, was that those who had medical
training estimated CPR's effectiveness
at 75 percent! In an effort to
understand why this would be so, the
authors examined a standard text used
to train health care workers and found
only a brief acknowledgement that CPR
was unlikely to be effective. The
handbook that the Red Cross uses to
teach its CPR classes to the public
did not confront the issue of low CPR
success at all. source
CPR in the real world
Q: Does CPR alone revive people?
A: No. But it depends on if the person receiving it was actually in cardiac arrest to begin with. And what was wrong with him in the first place.
As we've already seen, the effectiveness of CPR (when done correctly) varies widely, even when combined with other therapies.
Despite the development of electrical
defibrillation and the more recent
implementation of lay rescuer
defibrillation programs, the vast
majority of these victims do not leave
the hospital alive. In studies over
the past 15 years, only 1.4% of
patients with out-of-hospital arrest
in Los Angeles, Calif, survived to
hospital discharge; in Chicago, Ill,
the number was 2%, and in Detroit,
Mich, it was <1%. Conversely, a few
municipalities such as Seattle, Wash,
report much higher survival rates from
SCA—more than 15% in 1 study—which
suggests that survival rates need not
remain so low. Recent work in Europe
and elsewhere has confirmed that a
higher survival-to-hospital discharge
rate is indeed a realistic goal, with
survival rates as high as 9% reported
in Amsterdam and 21% in Maribor,
Slovenia. source
Given the innumerable causes which can lead to cardiac arrest, I obviously cannot address them all, however, there may be some instances when CPR alone can be lifesaving, or appear to the lay rescuer that it is lifesaving.
Recent revisions of standards by the American Heart Association no longer call for lay-people to perform a pulse check prior to initiating CPR if they find an unconscious victim who appears not to be breathing. So, the person receiving the CPR may not always be in cardiac arrest.
It's possible in these situations for the painful stimuli to rouse the unconscious (usually intoxicated) person in a manner similar to what is seen on tv. To the lay person and to bystanders without medical training, this would look exactly like what is pictured on tv.
Ventricular Tachycardia, Ventricular Fibrillation vs. True Asystole
The human heart requires both electrical and mechanical activity to pump blood effectively. A patient who is pulseless and not breathing may not necessarily be "flat-lined" and in certain cases, the inititation of CPR immediately may have an effect similar to that of a precordial thump(which is now reccomended in certain situations), in that the force of the impact induces an electrical stimulus which jolts the heart out of a non-perfusing rhythm.
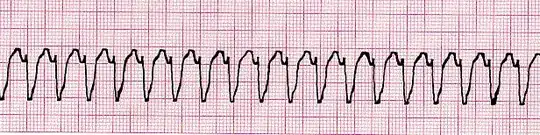
In Ventricular Tachycardia, the heart's electrical activity looks like this, but the person will often not have a pulse (because although the heart has electrical activity and some mechanical activity as well, it is inadequate to pump blood properly):
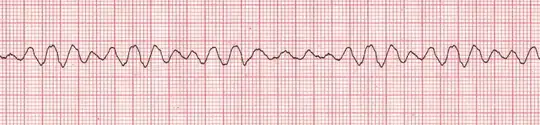
In Ventricular Fibrillation, the heart's activity looks like this, but the person will NOT have a pulse (again, because in this rhythm, the heart is unable to effectively pump):
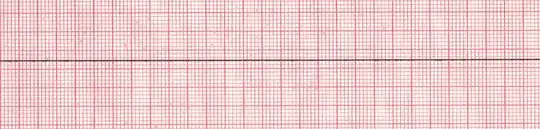
In true asystole (flatline) there is neither electrical nor mechanical activity in the heart:
However, without an EKG it is impossible to tell which rhythm a person's heart is in, and there is some chance (although probably quite remote) that the initial compression of CPR might jolt a person out of the first two, but not the third.
In reality, reversing a cardiac arrest is dependent largely on fixing the underlying cause.
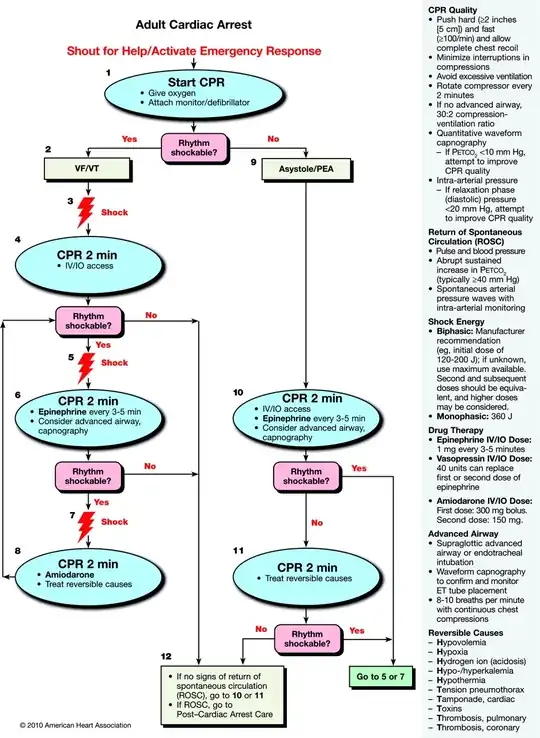
CPR is mainly effective by continuing to perfuse the body's tissues (especially the brain) with oxygen (and some other things), which will lessen damage and increase the chance of survival while other treatments (which are more effective at increasing survival rates) are administered. Typically, this involves electrical, drug, or surgical treatments. Although there are many variations, here is one example of an ACLS protocol for treating a cardiac arrest in full asystole, as you can see, it often requires much more than just CPR.
An often unaddressed factor in television is the potential for injuries caused by the CPR itself:
The most common injuries from chest
compressions are rib fracture (∼30
percent) and sternal fracture (∼20
percent). Other common
complications include aspiration,
gastric dilatation, anterior
mediastinal hemorrhage, epicardial
hematoma, hemopericardium, myocardial
contusion, pneumothorax, coronary air
embolus, hemothorax, lung contusion,
and oral and dental injuries.
The liver is the most commonly
injured intraabdominal organ, with
rupture occurring in about 2 percent
of cases. The spleen is infrequently
injured and ruptures in less than 1
percent of resuscitation attempts.
Rare injuries (incidence less than 1
percent) include tracheal injuries,
esophageal rupture, gastric rupture,
cervical spine fracture, vena caval
injury, retroperitoneal hemorrhage,
and myocardial laceration.
Complications may occur even with
properly performed CPR, especially rib
and sternal fractures. The possibility
of injury should not deter the
vigorous application of CPR, since the
outcome without effective
resuscitation is certain death.
Life-threatening injuries from CPR,
such as laceration of the heart or
great vessels, are rare. Proper
techniques will lessen the incidence
of serious complications. source
Q: Is CPR actually effective on someone who breathed water?
A: Sometimes, but not as often as television would have you think.
There is some debate about the effectiveness of rescue breathing in CPR, and in fact, lay rescuers are now taught a compressions-only method.
The role of rescue breathing is
currently debated; however, it is
likely important in prolonged arrests
or those of non-cardiac etiology.
Current recommendations encourage
inclusion of rescue breaths by trained
responders, but allow for elimination
of rescue breathing and emphasis on
chest compressions for responders
untrained or unconfident in rescue
breathing.source
A study done in a lifeguarded waterpark environment yields the following information:
Analysis of 63,800,000 guests with
56,000 rescues and 32 LSR rescues
shows that children and shallow water
both had relatively high levels of
rescues [62.6% for children aged 1-12
years and 42% for water depth less
than 1.52 m (5 ft)] and LSR rescues
[53.2% for children aged 1-12 years
and 65.6% for water depth less than
1.52 m (5 ft.)] with 87.5% of the LSR rescues resuming spontaneous
respiration and 75% having a poolside
neurological rating of Alert. source
The numbers here seem to indicate a much more impressive success rate than demonstrated above with CPR, but to understand how this works, it's important to understand the physiology of drowning.
The data appears favorable, mainly because these victims are often unconscious, but not yet in cardiac arrest. Also, the age of the patient, time spent without oxygen, and many other factors can affect survival rates.
When water enters the lungs the
victim's blood chemistry is rapidly
altered, often leading to heart
failure. In fresh water drownings
inhaled water is immediately absorbed
into the blood causing hemodilution.
The diluted blood quickly leads to
heart failure due to ventricular
fibrillation, a condition simply
described as shivering of the heart,
or anoxia (oxygen starvation). Sea or
salt water creates the opposite
effect. Water is drawn from the blood
into the lungs. This process causes
the blood to become more concentrated,
leading to an increased load on the
heart and heart failure. Older
drowning victims may experience
immediate heart failure as a result of
the initial trauma of drowning,
particularly in extremely cold
water.source
How does the drowning process happen?
A very basic outline of the drowning process:
- Panic and violent struggle to return to surface
- Period of Calmness
- Swallowing of fluid, followed by vomiting
- Terminal Gasp
- Unconsciousness
- Possible Seizures
- Death
*The time that this takes is variable, but it could be as little as 12 to 20
seconds from the first panic to unconsciousness. source
A book on forensic pathology details the process a little more delicately:
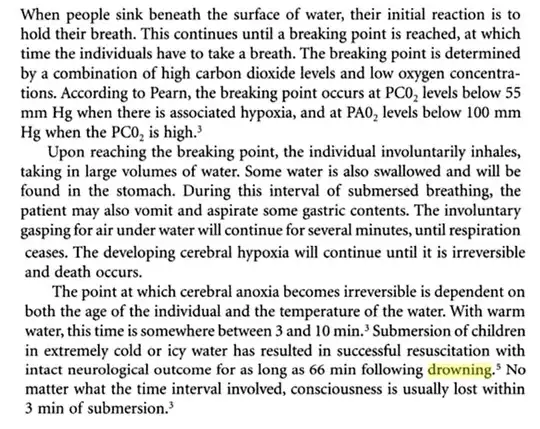 source
source
So, it could be argued that (since we have no way of knowing) some of the drowning victims portrayed in shows like Baywatch are in the very earliest stages of drowning and have only gone unconscious rather than gone into cardiac arrest, which would make their resuscitation plausible.
However, it does seem awfully convenient that they often revive their victims consistently in the most dramatic (yet, consistently vomit-free) way possible. Again, as it would seem is often the case with television and film, those telling the story tend to cherry-pick the most convenient and plot-friendly aspects of CPR.
